
Sleep Apnea: Diagnosis and Treatment
Physical Health

Sleep apnea is a serious breathing disorder that occurs during sleep. The affected person suffers repeated episodes of “apnea” (a temporary stoppage in breathing), which seriously disrupts the quality of sleep. The result can be non-restorative sleep, causing daytime fatigue, poor concentration, irritability, headaches, and reduced quality of life. Sleep apnea may also cause heart problems, such as serious arrhythmias (heartbeat irregularities).
In this article, we’ll talk about what sleep apnea is and how you might know if you have it, and we’ll focus on its diagnosis and treatment.
Types of Sleep Apnea
There are three types of sleep apnea, based on their cause: obstructive sleep apnea, central sleep apnea, and complex sleep apnea.
Obstructive Sleep Apnea
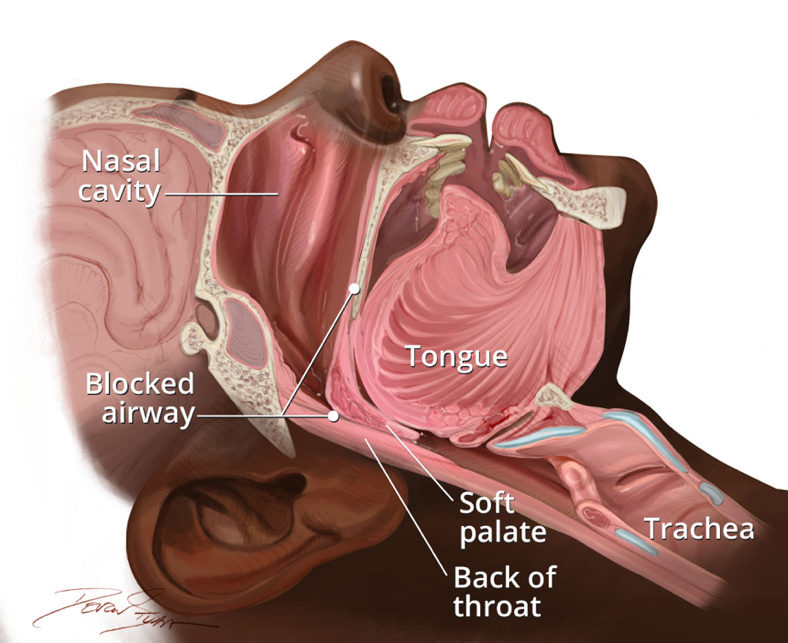
Obstructive sleep apnea (OSA) occurs when the body tissues in the upper airway repeatedly collapse during sleep (see Figure 1). The sleeping person experiences a narrowing or collapse of their upper airway while they inhale, causing either insufficient oxygen intake (hypopnea) or complete blockage of breathing (apnea). The most common reasons for the excessive tissue and/or muscle relaxation that bring on OSA are obesity, the use of alcohol or other sedatives, having abnormally large tonsils or other anatomical structures, and genetic vulnerability to OSA.
Figure 1. Obstructive sleep apnea (OSA) occurs when the soft tissues in the back of the throat, the soft palate, and the tongue block air from getting from the mouth and nose to the trachea during sleep.
OSA is by far the most common cause of sleep apnea, and it’s a very common disorder. Many cases go undiagnosed, but it’s estimated that in the United States (US), about 25% to 30% of men and 9% to 17% of women would meet the diagnostic criteria for OSA.
Central Sleep Apnea
Central sleep apnea (CSA) occurs when the brain intermittently fails to signal to the body to breathe during sleep, resulting in brief episodes of apnea. There are a variety of causes of brain-centered apnea, including drug use (especially opioid narcotic drugs, such as oxycodone, codeine, or heroin), being at high altitude, congestive heart failure, certain brain diseases (such as stroke or Parkinson’s disease), or primary (CSA with no obvious cause).
CSA is rare compared to OSA, comprising only about 2 to 3% of all cases of sleep apnea.
Complex Sleep Apnea
Complex sleep apnea occurs when someone who is on treatment for OSA begins developing symptoms of CSA. Because of this, it’s also known as “treatment-emergent CSA.”
Symptoms of Sleep Apnea
Many people with sleep apnea remain oblivious that they have a treatable breathing disorder. People generally do not wake from sleep during bouts of apnea, and the daytime symptoms may arise and worsen gradually, so that the person may think they’re tired all the time for any of a variety of reasons, such as stress, not enough sleep, or thyroid issues.
Typical symptoms of sleep apnea may include the following:
- Loud snoring, choking, or gasping during sleep, or apnea during sleep—these symptoms are usually observed by the person’s partner
- Excessive daytime sleepiness (see Figure 2)
- Non-restorative sleep (not feeling refreshed upon awakening in the morning)
- Insomnia
- Nocturnal acid reflux (acid regurgitation at night)
- Headaches, especially in the mornings
- Irritability, poor concentration during the day
- Nocturia (losing control of one’s bladder during sleep)
CSA is usually accompanied by less nighttime snoring, which is a central feature of OSA. CSA may also be accompanied by symptoms of the underlying neurological disorder causing it, such as a tremor in persons with Parkinson’s disease.
Figure 2. The non-restorative sleep and daytime sleepiness that often accompany sleep apnea can cause significant difficulties in your day-to-day function.

Diagnosis of Sleep Apnea
People don’t usually visit the doctor and say, “I have sleep apnea.” In most cases, they’ll complain of daytime tiredness, or non-restorative sleep, or that their spouse is complaining about their snoring. In such cases, these complaints should trigger the doctor to consider sleep apnea as a possible diagnosis.
The doctor will start by taking a history and asking about supportive information, such as:
- Symptoms suggestive of sleep apnea
- Medical history of conditions associated with CSA (such as previous stroke)
- Sleep patterns and habits
- Family history of sleep apnea
- Results of any previous testing that was done for sleep apnea
The doctor will also examine you to check on some things that may suggest a diagnosis of sleep apnea, such as:
- Your body mass index (BMI). Obesity is the most common physical finding in OSA, and a BMI greater than 35 kg/m2 is suggestive of OSA.
- Your neck circumference (a large neck is suggestive of OSA, especially a neck circumference of 17 inches or greater in males and 16 inches or greater in females).
- Your jaw and oral cavity, looking for abnormalities or excessive size in your jaw, tongue, tonsils, and throat.
- Your heart, to look for abnormalities that could cause or result from sleep apnea.
Figure 3. A large neck circumference is a risk factor for OSA.

Your doctor may also arrange for blood testing at the lab. They may do testing for diabetes, thyroid gland problems, blood counts, and other factors that may contribute to sleep apnea.
Screening Tests
Sleep apnea often goes undiagnosed for a prolonged period because the individual may not be aware of their nighttime symptoms unless they have an astute sleep partner. Also, daytime fatigue is one of the most common symptoms seen by primary care providers and has a long list of causes.
Healthcare providers often rely on the “STOP-BANG” questionnaire to screen patients they suspect may have OSA. The STOP-BANG is 90% to 96% sensitive at detecting OSA of any severity, and a positive result may indicate a need for further diagnostic testing. The questionnaire consists of 8 questions:
- Snoring: Do you snore loudly (louder than talking or loud enough to be heard through closed doors)?
- Tired: Do you often feel tired, fatigued, or sleepy during the daytime?
- Observed: Has anyone observed you stop breathing during your sleep?
- Blood pressure: Are you currently being treated for high blood pressure?
- BMI: Is your BMI greater than 35 kg/m2?
- Age: Are you age 50 or older?
- Neck circumference: Is your neck circumference greater than 40 cm (15.7 inches)?
- Sex: Are you male?
The STOP-BANG questionnaire is scored as follows:
- Answering yes to 2 or fewer questions = low probability of OSA
- Answering yes to 3 or 4 questions = moderate probability of OSA
- Answering yes to 5 to 8 questions = high probability of OSA
Anyone answering yes to 3 or more questions should probably be screened for OSA by a sleep study. However, the questionnaire is simply a screening tool; your healthcare provider should use their own judgment in deciding whether you require further testing. If your doctor suspects sleep apnea, they may wish to arrange for an overnight screening test that you do in your own home, of which there are two types:
Overnight oximetry test. This is a simple test in which you wear an oximeter (a device that measures your blood oxygen levels—see Figure 4) on your finger while you sleep for one night. If the device detects repeated dips in your blood oxygen levels, then it suggests sleep apnea, and your doctor will likely refer you to a sleep clinic for a definitive diagnosis.
Figure 4. A person undergoing an overnight oximetry test. The test involves wearing a simple blood oxygen monitor on your finger with an attached recording device while you sleep for one night.

The home sleep apnea test (HSAT) is a little more involved than overnight oximetry. The HSAT involves wearing a nasal sensor to monitor your airflow, a chest belt to monitor your breathing movements, and the same finger probe oxygen sensor that is used for overnight oximetry (see Figure 5). Like overnight oximetry, the HSAT is done during a single night of sleep, and a positive result will lead to a referral to a sleep lab for a definitive diagnosis.
Figure 5. The home sleep apnea test (HSAT).

Diagnostic Tests
Referral to a sleep lab for a definitive diagnosis of sleep apnea usually follows initial screening by your healthcare provider, including overnight oximetry or the HSAT. The sleep lab will perform a test known as “level 1 polysomnography” (PSG), which requires you to spend the night at the sleep lab. PSG is the gold standard test for diagnosing all three types of sleep apnea.
During the PSG test, a technician will hook up the monitors required by the test and monitor your readings (from a separate room) while you sleep. The results of your readings will be interpreted by a physician who is specially trained in sleep medicine, and they will review the results with you and communicate your diagnosis, if any.
The PSG test is complex and involves the following monitors (see Figure 6):
- Electroencephalogram (EEG): leads attached to your scalp to monitor your brain activity
- Pulse oximetry: the same finger probe used in overnight oximetry and the HSAT
- Temperature and pressure sensors to detect nasal and oral airflow
- Respiratory impedance plethysmography (RIP) belts around the chest and abdomen: these monitor chest and abdomen movements related to breathing and provide a measure of lung inflation and deflation as you breathe
- An electrocardiogram (ECG) lead that monitors your heart’s electrical activity
- Electromyogram (EMG) sensors to detect muscle contractions in your chin, chest, and legs
Figure 6. Level 1 polysomnography (PSG), a test performed at a sleep lab with multiple monitors attached to your body.

Treatment of Sleep Apnea
People with sleep apnea usually report dramatic changes to their day-to-day life once their sleep apnea is being treated. Typically, they notice sudden improvements in their energy levels, ability to concentrate, and overall quality of life.
If applicable, lifestyle modifications may be part of the treatment. For example:
- Weight loss to reduce tissue size in the neck and oral cavity
- Avoiding alcohol and other sedatives
- Sleeping on your side rather than your back
- Using an oral appliance while you sleep
- Regular exercise to improve breathing and promote a healthy weight
- Treating nasal congestion, such as from allergies or a deviated nasal septum
- Orofacial therapy: exercises to strengthen the muscles in your face and oral cavity
- There are devices available that use electrical nerve stimulation to strengthen the tongue
Surgery may be considered in severe cases. Surgery may include removing the tonsils or adenoids, debulking the soft tissues in the back of the throat, or jaw advancement.
The gold standard treatment for OSA and the obstructive component of complex (mixed) sleep apnea is continuous positive airway pressure (CPAP), which involves using a masked device to deliver continuous pressure to keep your airway open while you sleep (see Figure 7).
Figure 7. Continuous positive airway pressure (CPAP) for OSA treatment. The machine (bottom right) connects via a hose to a mask that’s worn over the nose during sleep.

Treatment of CSA is usually more challenging. The underlying cause should be addressed, and this may require a multidisciplinary team. For example, treating heart failure or tapering off opioids would be appropriate if either was determined to be a causative factor. Positive airway pressure (PAP) machines are usually used while the underlying cause is addressed or if it cannot be fixed. These may include one of the following:
- CPAP (as in OSA)
- Bilevel positive airway pressure (BPAP): This device is similar to CPAP but involves varying the airway pressure and requires wearing a mask over the nose and mouth.
- Adaptive servo ventilation (ASV): This is a smart device that senses the need for airway pressure and delivers pressure only when needed.
Sometimes, supplemental oxygen therapy is needed for CSA, particularly if there are heart problems involved.
Take-Home Message
Sleep apnea—especially OSA—is a common but underdiagnosed serious breathing disorder of sleep. It can cause significant symptoms that interfere with function and quality of life, but it is usually easily diagnosed and treated.


